| Full Presentation
of Fractures of the Wrist
Fractures of
the wrist are very common injuries. Around one quarter of all
patients in a Fracture Clinic will have suffered a fracture of the
wrist.
Fractures of the wrist are commonly given names after
the Doctors who first described them. The commonest type is a
COLLES’ fracture but you may also hear terms such as SMITH’S and
BARTON’S fracture. These days, Orthopaedic surgeons tend not to use
these terms but to classify these fractures according to their
prognosis, that is how severe the injury to the bone and wrist joint
is.
There are many classifications for fractures of the
distal radius. One of the commonest is that according to FRYCKMANN
who is a Swedish Orthopaedic Surgeon who described a fracture
classification system based upon the parts of the joint that were
involved. What he says, and this has been borne out by experiments
since this time, is that the more parts of the joint surface that
are involved, the more likely the fracture was to result in a poor
outcome.
The usual cause of a fracture of the wrist is a fall. The person
falling tries to break their fall by putting their hand out to save
themselves and in doing so, the wrist is forced backwards (figure
one).

Figure one: A fall onto the
outstreched hand is the usual cause of fractures of the wrist joint. Click here to view a larger version.
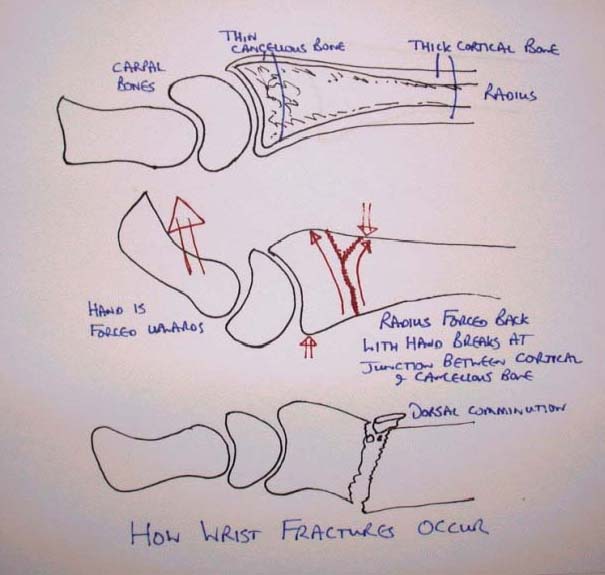
The break or fracture usually occurs about 2.5cm from
the wrist joint at the point where the radius (the largest of the
two bones of the forearm) starts to narrow to form the broad and
relatively soft (concellous) bone forming the joint to the hard
(cortical) bone in the shaft of the radius (figure two).

Figure two: How and why wrist
fractures occur. Click here to view a
larger version.
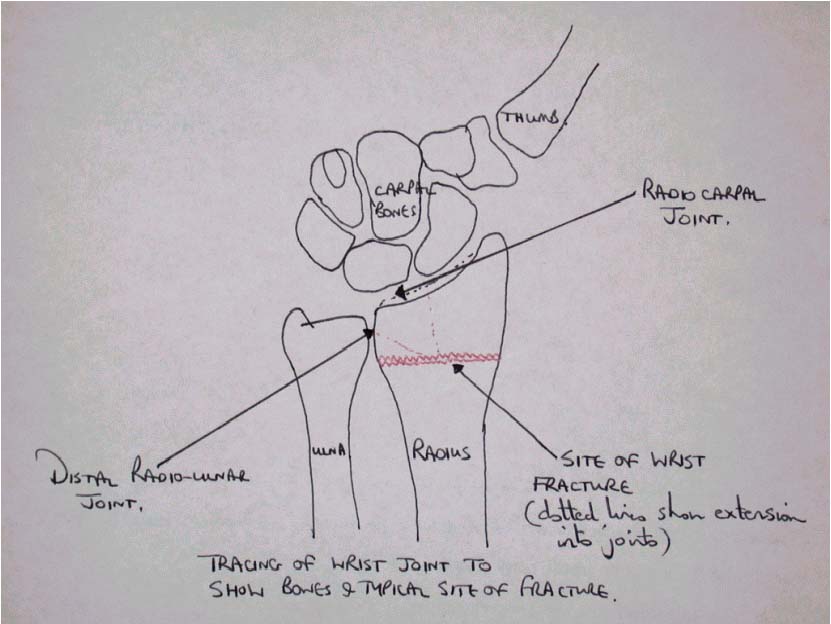
With more severe force the fracture may extend into
either or both of the main joints which allow the wrist to move.
These joints are the radio-carpal joint and the distal radio-ulnar
joint (figure three). When fractures involve joints (what is
known as an intra-articular fracture) they can cause stiffness of
the joint and if the surface of the joint becomes uneven, this may
result in arthritis of the joint. There is another problem
associated with wrist fractures which is that there are two bones
that make up the wrist joint, the radius and the ulna. In most
people these bones are approximately the same length (figure
three).

Figure three: Tracing of a normal
wrist seen from the front to show normal features and the site of fracture. Click here to view a larger version.
When a fracture of the wrist occurs
the commonest scenario is that the radius will become short when
compared to the ulna. This is because the dorsal comminution
(see figure two) results in a space into which the radius can
settle back as the fracture heals. This results in shortening of
the radius in comparison to the ulna and the ulna may then
effectively become longer so that when the wrist moves it causes
pain and restriction of movement.
The commonest form of fracture of the wrist causes
the radius to bend away from the palm. The patient may therefore
notice a change in the shape of the wrist which is called the
“dinner fork” deformity after its shape. This is a deformity of the
COLLES’ fracture (figure four).

Figure four: Wrist fracture (X-ray)
seen from the side view to show "dinner fork" deformity of Colle’s
fracture. Click here to view a larger
version.
It is usually
obvious to the patient following a fall once a fracture of the wrist
has occurred, the wrist joint is usually very painful and swollen
and it may of course be deformed. Immediate treatment consists of
resting the painful part (for example in a sling). The use of
something cold will help control swelling, ice or frozen peas are
suitable but they should always be wrapped
in something (e.g. a towel) and NEVER applied directly to the skin.
This is because direct contact with ice may cause skin damage to
occur.
Medical advice should be sought immediately and it is
important to remember that the patient may require an anaesthetic
for treatment of these fractures and it is therefore important to
avoid food and drink until a Doctor or other Medical Practitioner
has seen the injury so as to avoid a delay in treatment.
Almost always an X-ray
(radiograph) of the wrist is required to make an accurate diagnosis
of wrist fractures and to decide upon the correct treatment.
Figure four shows the typical appearance of a wrist fracture (in
this case a COLLES’ fracture). This X-ray shows that the radius has
both bent and moved away from the palm. It is this movement (what
Orthopaedic surgeons call angulation and displacement) which causes
the dinner fork deformity.
Figure four: Wrist fracture (X-ray)
seen from the side view to show "dinner fork" deformity of Colle’s
fracture. Click here to view a larger
version.
Leaving the fracture in this
position (figure five) will almost certainly result in the
problems mentioned above, particularly if the radius remains short
compared to the ulna. For this reason, this fracture will almost
certainly require further treatment.

Figure five: X-ray of
Colle’s fracture seen from the front to show that the radius becomes shortened.
Click here to view a larger version.
There are three parts to the
treatment of a fracture of this sort, firstly to reduce the
fracture, that is to put the two parts of the fracture back to their
original position. Once the fracture is reduced, it needs to be kept
in the correct position until the bones have a chance to heal, this
on average takes about six weeks. The third part of fracture
treatment is to ensure that the soft tissues of the arm are kept
mobile until the arm can get back to its original use.
There are many methods of treatment for fractures
of the wrist and it is true to say that Orthopaedic surgeons are
undecided as which method of treatment is best. The particular
method of treatment will depend both upon the preference and
experience of the surgeon and will also depend upon the nature of
the fracture. Most surgeons will use a variety of methods to treat
fractures of the wrist. It is also worth saying that traditionally
treatment of these fractures has been guided by the statement of
COLLES in his original paper who said that people with these
fractures do well even if the fracture isn’t reduced. This has meant
that these fractures have tended to be under treated in the past
although most Orthopaedic surgeons now realise that treatment of
these fractures is important if later problems are to be avoided.
This is particularly true these days when patients place greater
demands upon their wrists and are less willing to accept limitations
of movement and/or pain. Experimental studies which have looked at
these fractures have demonstrated that approximately 97% of
fractures are of the COLLES’ type i.e. the deformity is away from
the palm and about 3% are towards the palm, that is the SMITH’S type
of fracture.
Reduction of the fracture may be achieved by
manipulation of the fracture, that is pulling on the hand to pull
the bones back into place. This is commonly performed in the
Anaesthetic Department or Emergency Room and whilst general
anaesthesia may be used for this, it is more common to do it by some
means of local anaesthetic block or by injection of local
anaesthetic into the fracture site (what is known as a haematoma
block). Once the fracture has been reduced, it is often maintained
by use of a plaster applied to the arm, a so called COLLES’ plaster.
Instead of a full plaster, a backslab is often used in the early
stages after injury, that is a plaster which as its name suggests
consists of a slab of plaster which does not completely encircle the
limb and so, although it protects the injured area and maintains the
reduction, allows the arm to swell as it is likely to do in the
early stages.
If your Orthopaedic surgeon decides that plaster
treatment alone is suitable for your fracture, it is important
particularly in the early stages to elevate the limb but more
importantly, to get the affected limb mobilized, not just the
fingers and thumb but also the elbow and shoulder as these will
often give problems in the long term.
If however the
treating surgeon feels that plaster treatment will not control the
fracture then he or she may decide that operative treatment is
appropriate. The options which may be considered include:
| 1. |
Fixing the fracture in
position with stainless steel wires ("K" wires). |
| 2. |
Using an external fixator in which pins are
drilled into the bone either side of the fracture and connects
to a stabilising device outside of the body. |
|
3. |
Opening the
fracture and fixing it in place with screws and plates. These
screws and plates may be made of metals such as stainless steel
or titanium or materials which the body is able to absorb (so
called reabsorbable plates). |
|
4. |
Intra-medullary
devices. These are devices which are inserted into the inside
of the bone through a small opening in the radius (the main bone
of the arm) which are then fixed in place with screws to prevent
the fracture from moving. |
Whichever method is chosen,
because the bone tends to splinter at this site (what Orthopaedic
surgeons call comminution), any of the methods mentioned above may
be combined with filling the space that becomes apparent when the
fracture is reduced i.e. moved back into position, traditionally
this was achieved by using bone taken from the pelvis (bone graft)
or by sterilised bone from other materials or other sources of bone
mineral e.g. coral. These days it is more common to use bone
substitutes,
these consist of the mineral content of bone
which is made into a form which allows it to be injected into the
fracture site.
More recently, if internal fixation is used i.e.
insertion of plates and screws into bone, they are often what is
known as angularly stable i.e. unlike earlier versions of plates,
the screws are fixed into the plate (usually this is achieved by a
thread in the screw which screws into the plate itself). This makes
the plate and screws what is known as “angularly stable”. The
benefit of this is that it prevents the lining of the joint or
articular surface falling back into the space and more importantly,
may often these days mean that bone graft is not required.
There are advantages and disadvantages to each of
the methods mentioned above, but it is increasingly recognised that
it is this splintering of the bone which occurs on the top of the
wrist (dorsal comminution) which is the key to preventing the
fracture re-displacing (that is returning to its fractured/broken
position) whilst the bone heals. The advantages and disadvantages of
each method are indicated in the table below:
Advantages and Disadvantages
| Method |
Plaster/brace |
| Advantages |
Easy to apply Operation not required |
| Disadvantages |
Movement of the hand may result in
loss of position of the fracture especially as swelling goes down
Plaster needs to be kept on for six weeks and so wrist and hand stiffness
may result
Plaster cannot control dorsal comminution |
| |
| Method |
"K" wires |
| Advantages |
Technically simple operation |
| Disadvantages |
Because "K" wires are smooth
they are not good at preventing loss of fracture position
A
plaster is still required and stiffness of the wrist may result
As the pins are often left out of the skin infection is a common
complication
Insertion of wires may result
in damage to the tendons around the wrist joint |
| |
| Method |
External fixation |
| Advantages |
Fracture is
reduced by pulling onto the wrist ligaments (what is knows as
ligamentotaxis) without opening up the fracture
Certain
types of fixator include hinges which allow the wrist to move
(and hence help to prevent stiffness) with the fixator on whilst
keeping the fracture in place |
| Disadvantages |
Fixators are often bulky and unsightly
The nature of the wrist ligaments means that
to keep the fracture in place wires, screws or bone graft may
also be needed in addition to the fixator
If the fixator is applied with too much pull
(traction) the wrist or hand may become stiff
The pins
which attach the fixator to bone may become infected (pin site
infection) |
| |
| Method |
Bone Grafting |
| Advantages |
Use of bone
which includes the strong outer layer of the bone (the cortex)
means that this method is strong enough to hold the fracture in
place and prevent loss of position due to dorsal comminution
(see above)
Combining
this with the softer inner bone (cancellous bone) stimulates the
fracture to heal very quickly |
| Disadvantages |
Other methods
such as K wires or screws or even plates may be needed to hold
the graft in place
Bone from
the cortex can usually only be obtained from the pelvis, this is
the main problem as the site from which the bone is taken may be
very painful and result in difficulty in walking for several
weeks |
| |
| Method |
Internal fixation (use of plates and screws) |
| Advantages |
The
greatest advantages of metal plates and screws is that they are
strong enough to fix the fracture in position and this allows
the wrist to be mobilized quickly and often a plaster is not
required
Since the advent of angularly stable implants
which hold the articular surface or lining of the joint in its
correct position, there is less chance of the fracture sinking
back into the space behind the joint and the need to add other
parts to the operation such as using bone graft or bone
substitutes (as described above) is less likely unless the
fracture is extremely unstable
There are
now several different ways in which the wrist may be plated and
these are described below including bioabsorbable plates. |
| Disadvantages |
Plating
of the wrist is a technically difficult operation and inevitably
there is a scar on the wrist
The tendons (leaders) around the wrist joint
are close to the site of the fracture and when metal plates are
used these tendons may become irritated by the plates (what is
known as synovitis) or they may even rupture
The
presence of plates around the wrist may result in discomfort for
the patient in the long term and therefore another operation may
be required to remove the plate itself. |
| |
|
Method |
Intra-medullary
devices |
|
Advantages |
The scars are
smaller than with traditional open reduction and internal
fixation |
|
Disadvantages |
Intra-medullary
devices are most suitable to extra-articular fractures i.e.
those where the joint surfaces are not involved and this
represents a relatively small proportion of distal radial
fractures
These
devices have not been used long enough to demonstrate that they
offer advantages over the current methods |
At Southend Hospital we have been
using bioabsorbable plates (Figures six and seven) over the last
seven years. These plates offer the advantages of metal plates in
that they are strong enough to fix the fracture well enough to allow
immediate mobilization but unlike metal plates they are broken down
by the body after about three months and so will help to avoid the
problems with the tendons which occur with metal plates. These
plates are combined with bone substitutes. We have now published the
results of our use of bioabsorbable plates in a peer-reviewed
Journal, the Journal of Hand Surgery, and we have also published
other papers which demonstrate the technique in terms of the
approach to the wrist which we use.

Figure six: Reunite reabsorbable plate on
plastic bone model; note that these plates are not visible on X-ray. Click here to view a
larger version.

Figure seven. Reunite plate and
Biobon in a fracture of the wrist (The plate is not visible on X-ray but the holes for the
screw are). Click here to view a
larger version.
Over the last four or five years it has become more popular to
approach the wrist from the volar surface, that is the palmar
surface of the wrist. The advantage of this approach is that it
avoids some of the problems associated with having a plate on the
back of the wrist. Since these angularly stable plates have been
available, this approach from the palmar side of the wrist has
become much more popular. Whilst this method offers advantages in
terms of the fact that there is less chance of tendons being
irritated due to the fact the plate is applied to the volar side of
the wrist, that is the palmar side where there are far fewer
tendons, because the screws which are used have to come through to
the dorsal or top side of the wrist there is still the potential for
irritation of tendons. For patients where there is involvement of
the joint surfaces it is sometimes difficult to see and reduce (that
is put back into place) the joint surfaces from the volar side which
limits the use of this approach.
There are now also special plates which can be
applied to the specific parts of the wrist which are broken, what is
called a column approach. This means that smaller plates may be
applied to specific fragments within the wrist and these can be very
useful for particular fracture patterns.
From what has been said
above it will be obvious that there is no one best method for the
treatment of fractures of the wrist. Each fracture needs to be
judged upon its merits and there may be a variety of treatment
methods which are available depending upon the type of fracture and
the demands placed upon the wrist by hand dominance, occupation or
leisure interest. It is also important to realise that each
Orthopaedic surgeon will have a method or methods of treatment which
they are familiar with and which will work for them.
If you are
unlucky enough to suffer a fracture of the wrist, the most important
thing in treatment is to find a surgeon who understands and has an
interest in wrist fractures and who takes an interest not just in
the bones or soft tissues but also in the after care and what your
demands upon the wrist are likely to be. You might consider asking
your surgeon the following:
| 1. |
What arrangements are there
for aftercare once the operation has been performed or the plaster removed? |
| 2. |
If an operation is
suggested, who is going to perform it and what is their experience with the method
suggested. |
| 3. |
If an operation is proposed
will it allow me to mobilise (move) the wrist more quickly than if I opt for plaster
treatment. |
| 4. |
What can go wrong with this
treatment method and what can be done to correct it should this happen. |
The commonest problem
following fractures of the wrist is mal-union, that is when the
radius heals in the wrong position. As indicated above this is
usually due to the fact that the broken part of the radius falls
back into the hole on the back of the wrist left by the dorsal
comminution. This often results in the radius being shorter than the
ulna and is often combined with tilting backwards of the wrist. This
results in both deformity (the wrist appears misshapen) and pain due
to the ulna catching on the bones of the wrist (the carpal bones).
If this occurs it is possible to correct this by means of surgery.
There are a number of methods used to achieve
this but in general terms they involve either re-breaking the radius
and returning it to its original shape or changing the ulna to make
it fit the new shape of the radius. Re-breaking the radius (known as
an osteotomy) will usually involve the use of a bone graft to hold
the bone in position until it heals and this is then supported by
either a plate or an external fixator. Since however angularly
stable devices have become available the use of bone graft is
becoming less common and it is my practice now to try and avoid bone
graft as these angularly stable implants are strong enough to allow
use of the plate alone without bone grafting. This is obviously
decided at the time of operation. The alternative to this is to
make the ulna shorter by removing a piece of bone and putting a
plate on it to hold the ulna in place until such time as it heals or
it may be matched to the size of the radius by trimming it to fit (a
matched ulna procedure). As can be imagined this is a specialised
part of Orthopaedic or Hand surgery and your surgeon may decide to
send you to a surgeon who has a specialist interest or experience in
this field.
One other
important part of wrist fracture surgery is that fractures of the
wrist are often associated with injuries to the ligaments of the
wrist. This can be quite difficult to diagnose in the initial
stages and either immediately after the fracture or at some time
later if there is the suggestion that the ligaments of the wrist are
involved, it may be necessary to further investigate this. There
are a variety of methods available to investigate wrist problems
further including further X-rays although these do not show soft
tissues or MRI and CT scanning. It is more common these days that
wrist surgeons will want to examine the wrist surface itself and a
common way to achieve this is by use of wrist arthroscopy when a
small device is inserted into the wrist using keyhole surgery to
examine the surface of the wrist joint and to assess the nature of
any damage to the joint surfaces and to the ligaments or to another
structure known as the triangular fibro cartilage complex (TTCC)
which has a similar structure to the cartilage of the knee and may
be damaged in a similar way. Wrist arthroscopy is a specialist form
of wrist surgery. It is however becoming a more commonly performed
operation these days. It is traditionally performed using a rigid
arthroscope. However, at Southend Hospital over the last two years
we have been pioneering the use of a flexible scope which is much
smaller than the current scope (approximately half the size) and to
give an idea of the sizes involved, the current scope used is 1.2mm
in diameter which is approximately the thickness of a 5 pence
piece. Our initial results with this procedure have been presented
at International Meetings including the International Federation of
Surgery for the Hand Meeting in Sydney, Australia in March of 2007.
The other advantage is that this method can be performed under local
anaesthesia if the patient does not wish to have a general
anaesthetic. |